The bottom line: The Language Access for All Act of 2026 is part of a real shift in how language access is regulated, measured and enforced. For most health systems, the standard is rising faster than the budget, the interpreter market or the staff bandwidth available to meet it. This piece is an honest read of what's changing, where the achievable gains actually are and where some gaps, particularly for rare languages, don't have a clean answer yet. We'd rather name that than pretend otherwise.
This blog piece is inspired by a live event by Piedmont Global in which Dr. Bill Rivers, Saba Dovlatabadi and Mary Grothe discussed the implications of the Language Access for All Act of 2026 for healthcare and other regulated industries.
Health systems did not design this regulatory environment. They are navigating it. Usually with thinner margins, harder staffing markets and longer procurement cycles than the pace of policy change assumes. The Language Access for All Act of 2026 raises the floor again. The question worth asking is not whether the standard is rising. It is what to actually do about it from where you are.
What is changing under the Language Access for All Act of 2026?
Language access has moved from a civil rights principle backed by Executive Order 13166 to an enforceable operational standard backed by statute, with measurable AI accountability and public reporting.
Three things are happening at once:
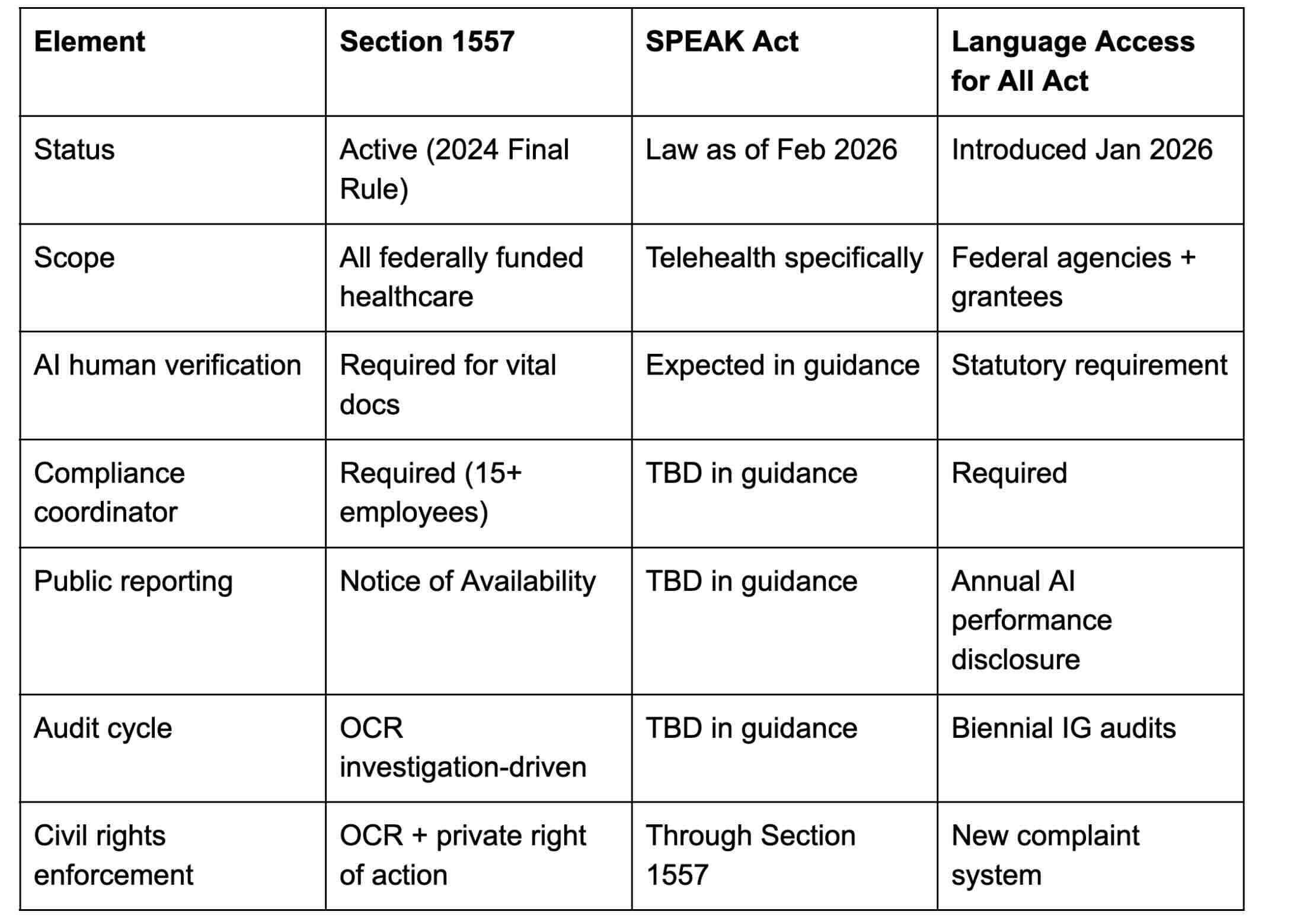
The legal framework is hardening. The 2024 Final Rule of Section 1557 sharpened the existing baseline. The SPEAK Act became law in February 2026 and sets a February 2027 deadline for HHS telehealth language access guidance. The Language Access for All Act of 2026 (H.R. 7223) is moving through Congress with the most specific AI accountability standards yet proposed.
AI is now in scope, with specifics. The Language Access for All Act would require qualified human verification of AI output, annual disclosure of error rates and confidence levels and biennial Inspector General (IG) audits.
The deadlines are real. Procurement cycles are long enough that February 2027 is already inside the window for most systems.
We're not going to walk through each law in detail. Others have done that well. The strategic frame matters more.
How do the three language access laws fit together?
Comparison and Compliance
What is the real tension between compliance pressure and available language access resources?
Most healthcare leaders we talk to already understand that language access matters. They are not convinced by lectures about civil rights. They are working within real constraints:
A finite budget that the regulatory pressure does not adjust for
An interpreter market that is uneven by language and time of day
Clinical staff already stretched on multiple compliance fronts
Telehealth platforms procured before language access was a procurement criterion
Smaller facilities with the same legal obligations as flagship hospitals and a fraction of the resources
The honest framing is that the standard is rising faster than the means available to meet it. That tension is real. Pretending otherwise (on either side) does not help anyone.
What we can do is be specific about where progress is achievable, where the work is harder and where the gaps don't have a clean answer yet.
How should health systems plan for the LEP populations they serve?
Before evaluating technology, vendors or AI vs human, the most useful work is usually the most basic: getting clarity on who actually walks through the doors of each facility, in what language, with what literacy levels and at what frequency.
This sounds obvious. It rarely happens at the right level of granularity.
Why does aggregate LEP data fall short?
Most language access strategies default to one of two shortcuts: the state-level top-15 list required for Notice of Availability, or the system-wide aggregate. Both miss the operational truth. A health system with multiple facilities serves dramatically different populations, and a uniform plan applied across all of them rarely reflects the reality on the ground at each site. Granularity at this level matters.
A concrete example: New York's hidden language gaps
During the Piedmont Global discussion, Saba Dovlatabadi pointed to a striking data point: New York State alone has approximately 2.5 million LEP residents, and the most pressing unmet language access gaps are not in the languages most healthcare organizations plan around.
Three languages Dovlatabadi flagged as significantly underserved:
Nepali: concentrated in Queens and increasingly across the boroughs
Tigrinya: spoken by Eritrean and northern Ethiopian populations along resettlement corridors
Mixtec, also known as Tu'un Savi: an Indigenous language of southern Mexico, spoken by Indigenous Mexican migrant populations across New York
These languages share a profile that makes them invisible in standard compliance planning. They rarely appear on state-level top-15 lists. Their speakers concentrate in specific neighborhoods, parishes and clinics. Qualified interpreter supply is thin and regionally concentrated. And the communities are growing faster than aggregate state data captures.
Medical institutions serving these communities should identify these gaps in their own patient populations and build a coverage plan for the rare languages their community actually speaks. New York is one example. Every state has its own version. Every health system has facilities where the local list looks nothing like the state aggregate.
What does granular population planning look like in practice?
Per-facility language demand modeling, refreshed quarterly
ACS census data combined with internal patient records
Service line segmentation: ED, oncology, behavioral health and OB-GYN often have very different language profiles
This is the foundation. Every downstream decision about contracting, AI and infrastructure is only as strong as the baseline it rests on. The goal is to filter as far down as possible, so the picture you're working from is close to what's actually happening on the frontline.
How large is the interpreter gap in US healthcare?
We've identified the gap. Now what?
This is where most language access pieces stop. We want to keep going, because the next question is the harder one, and it's the one that gets asked in real hospital operations meetings.
Interpreter Availability Is Not Uniform
Spanish: deep market, abundant qualified professionals across modalities
Somali, Hmong, Haitian Creole, Burmese: thin markets in most regions, often regional concentrations
Karen, Quiché, Akan, Marshallese, Tigrinya, Chuukese, Pashto, Mixtec/Tu'un Savi, Nepali: very thin national supply, significant gaps in evening, weekend and emergency coverage
For some languages, the qualified interpreter pool (anywhere in the country) is small enough that a 2 AM emergency department request will not be filled in time. This is not a vendor failure. It is a structural feature of the market.
What Do You Actually Do When No Qualified Interpreter Is Available?
This is the honest question, and it's the one most language access guides avoid.
You've done the population analysis. You've contracted with a reputable vendor. You've built the workflow.
And tonight, you have a Karen-speaking patient in the ED, and there is genuinely no qualified Karen interpreter available... anywhere, at this hour.
What do you do?
There is no clean answer.
This is not what compliance frameworks reward. It is what real access looks like at the edge of what's possible. Health systems doing this work in good faith deserve credit for the effort and a clear-eyed view of where the system itself is limited.
Where does No Barrier help and where does it not?
Language access is expensive. For a mid-sized health system, full coverage across the three-law framework can run into seven figures annually. The budget is finite. The regulatory pressure isn't.
We try to be specific about what we can help with and what we can't.
Where can No Barrier help?
Rare languages, not super-rare. It's worth separating the two. No Barrier offers accurate AI medical interpretation in Haitian Creole, Bengali, Burmese, Nepali, Urdu and other rare languages. These are rare compared to Spanish, but they are already in production with reliable accuracy, not on a roadmap.
Dialects, not just languages. Spanish is not one language in clinical practice. No Barrier covers five Spanish variants, from Mexican to Dominican to Puerto Rican, in a single connected device that delivers the capability of five human interpreters instantly. The same applies to French and Arabic.
On-demand language additions. Depending on volume and clinical need, our team can evaluate the resources required to add a new language to the 40+ we already support in AI medical interpretation.
Where does No Barrier not pretend to solve the problem?
Super-rare language scarcity. When no qualified Tigrinya, Mixtec (Tu'un Savi) or Marshallese interpreter is available in the country at 2 AM, no vendor (sometimes including AI medical interpretation, where the training data simply isn't there) produces one out of thin air. We can help you reduce the frequency of those moments and document them well when they happen. We cannot make them disappear.
The long-term interpreter pipeline. Building qualified interpreter capacity in thin-market languages is a multi-year, multi-stakeholder effort involving academic programs, community organizations, certifying bodies and federal funding. Vendors can support that work. We cannot replace it.
The funding question. Whether language access is adequately resourced as a public good is a policy question that sits above any operational solution.
The honest framing: we close the gaps we can close, and we help build a defensible, patient-centered approach to the ones that remain.
What is the quieter goal beyond language access compliance?
We've used the phrase "language access is a right" carefully in this piece, because we don't want to land on a moral high ground that doesn't help anyone do the work.
Here's the practical version of the same idea: the patients who need language access did not create the regulatory pressure, and they don't experience your compliance posture. They experience whether they understood the diagnosis, whether they could ask a question, whether they trusted the discharge instructions enough to follow them.
The systems that focus on those outcomes and use the regulatory framework as scaffolding rather than as the goal tend to do well on audit because they're doing well on care. The reverse is harder.
This is not a sermon. It's an observation from the work.
A Final Honest Note
The regulatory floor is rising and that's understandable. Patient lives are at stake. Language access is a right for everyone and rights need regulation to make sure they are not optional but actually implemented. The patient need has been there all along.
For health systems doing this work under pressure, the most useful response we can offer is not a list of obligations. It's a clear-eyed read of what's possible from where you are and a willingness to do the work alongside you on the parts we can actually solve.
That work has a clear shape:
Map the data. Which patients, which languages, which medical sites.
Build the framework and the protocols. When human, when AI, when both.
This is what it looks like to be compliant, honest and aware of the limitations the market has today.
And the market is moving. The technology will keep progressing and rare language capabilities will progress with it. What is structurally hard today will be operationally possible sooner than most planning cycles assume. The work right now is building the foundation that lets you take advantage of those gains when they arrive: clean population data, defensible protocols, a hybrid model that already knows how to absorb new capability without rebuilding from scratch.
If you're working through any of this and want to compare notes, our team at No Barrier maps coverage gaps with health systems regularly. We're happy to look at your population data and tell you, plainly, where we can help and where we can't.
FAQs
1. Is the Language Access for All Act of 2026 law yet?
No. It was introduced in the House in January 2026 and is in committee. Near-term passage is uncertain in a divided Congress. But the framework, particularly the AI accountability standards, is shaping the regulatory direction regardless of when or whether the bill passes.
2. Does Section 1557 apply to small clinics?
Yes. Any provider receiving federal financial assistance, including Medicare and Medicaid reimbursement, is a covered entity. The legal obligations do not scale with practice size, even if the resources do.
3. Can AI replace human interpreters under these laws?
No. Section 1557 already requires qualified human review for machine translation of vital content. The Language Access for All Act would make human verification a statutory requirement. AI is a permitted tool, not a substitute for qualified human accountability.
4. What is the most urgent action item for healthcare leaders right now?
Population mapping at the facility level. Without a clear picture of who is actually being served, in what languages, at which sites, every downstream decision about technology, contracting and AI rests on weak ground.
5. How do we handle rare languages when no qualified interpreter (human and AI) is available?
Honestly and with documentation. Exhaust the qualified pathway across vendors and time zones. Use the best available bridge with rigorous verification. Treat every gap as data that justifies long-term pipeline investment. There is no clean answer at the edge of the market, but there is honest work to do.
Eyal Heldenberg
Co-founder and CEO, building No Barrier
Eyal has 20+ years in speech-to-speech and voice AI and is the co-founder of No Barrier AI, a HIPAA-compliant medical interpreter platform. Over the past two years, he has led its adoption across healthcare organizations, helping providers bridge dialect gaps, reduce compliance risk and improve patient safety. His mission is simple: ensure health equity by removing language barriers at the point of care.